Obesity Value Is Shifting From Efficacy to Access
Most obesity pipelines are still trying to beat GLP-1 efficacy. That's no longer the game.

Download the Visual
Most obesity pipelines are still trying to beat GLP-1 efficacy. That's no longer the game.
The belief that value runs through efficacy alone made sense when the question was feasibility: could incretins deliver durable, meaningful weight loss at scale?
That question has been answered. Injectable GLP-1s have established a de-risked efficacy reference point. Not a hard ceiling, but a validated benchmark across multiple molecules and sponsors. Strategic uncertainty has shifted from whether meaningful weight loss is achievable to how it can be delivered, accessed & paid for at scale.
This is the part many pipelines miss: beating current efficacy benchmarks alone is no longer sufficient. A superior injectable faces the same payer scrutiny, access friction and incumbency advantages that constrain existing GLP-1s. The bottleneck has moved.
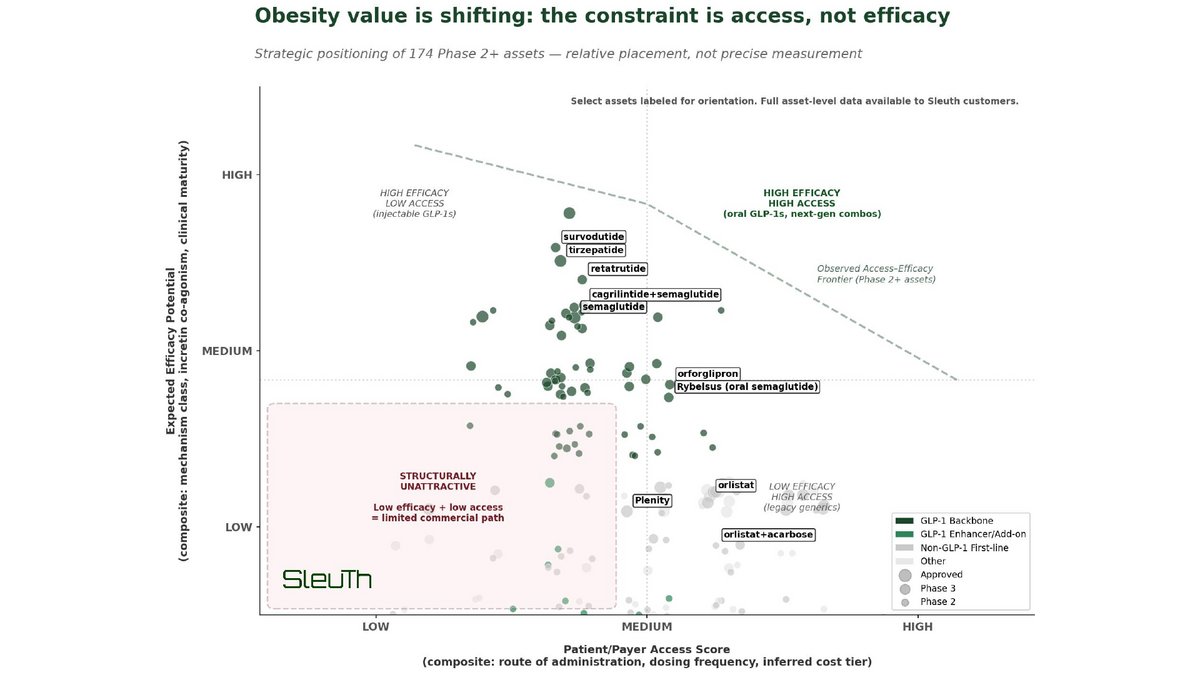
I used Sleuth to map 174 Phase 2+ obesity assets across two dimensions that matter for commercial viability: expected efficacy potential (mechanism class, incretin co-agonism, clinical validation) and patient/payer access (route, dosing burden, tolerability and inferred cost pressure). The result is an access–efficacy frontier. Not a theoretical performance race, but a real-world optimization problem.
The pattern is striking. Late-stage capital, BD interest, and Pharma portfolio focus cluster around assets that sit on or push the frontier. Assets far from it (particularly those low on both access and efficacy) face structural commercial headwinds regardless of scientific novelty.
Two distinct strategies are emerging to expand the frontier:
1. Oral GLP-1s like orforglipron and VK2735 illustrate horizontal expansion - not because all orals are inherently patient-friendly, but because select programs meaningfully relax specific access constraints while remaining close to the injectable efficacy reference. This isn’t a claim that efficacy no longer matters. It’s a recognition that, in a payer-managed category, access friction often becomes a key constraint once efficacy is de-risked.
2. Combo strategies like cagrilintide+semaglutide and amycretin attempt diagonal expansion, pairing efficacy preservation with differentiated tolerability, durability or muscle-sparing profiles. The bet is that selectively closing efficacy or tolerability gaps can unlock value even when access improves only marginally.
These are illustrative examples of strategic direction, not predictions of winners - the point is the framework. Frontier expansion does not require majority market share: even assets serving narrower segments can shape payer dynamics, portfolio strategy and capital allocation.
